ICD & CRT Implantation
Implantable Cardioverter-Defibrillators (ICDs):
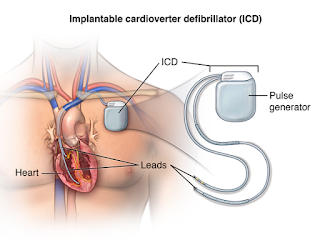
Implantable Cardioverter-Defibrillators or ICDs perform all of the features of a permanent pacemaker (such as treating slow heart rhythms) but they also have the capacity to treat dangerously rapid heart rates with rapid pacing or with shocks. They are implanted in the same way as a permanent pacemaker (PPM) with leads traveling down to the heart through a vein but the device itself is larger than a PPM and the lead that is capable of giving shocks is also a little larger (thicker) than a normal pacemaker lead. The device needs to be larger because shocks (or high voltage therapies) require more energy and more battery capacity than low voltage therapies like pacing the heart. A number of studies have shown that ICDs can save lives in patients who are survivors of a cardiac arrest or in patients who have a cardiomyopathy (heart muscle weakness) where the left ventricular ejection fraction is less than 35% (the normal ejection fraction or amount of blood the heart pumps with each beat is ≥50-55%) (1, 2). If an ICD is being implanted purely to treat a possible future cardiac arrest (and not to perform any pacing function) then it will not change your heart failure symptoms but is purely a treatment aimed at extending a patients life. Treatments aimed at directly targeting rapid heart rates to improve symptoms are often needed in combination with an ICD (these include medications or ablation procedures). Potential complications with ICD implantation include a 1:300 risk of bleeding around the heart that may require drainage, a 1:100 risk of injury to the lung as the leads are passed through the vein at the top of the lung and a 1-2% risk of bleeding or infection. If any complications do occur they will generally be identified and treated at the time of the procedure. All current ICDs are compatible with ‘home monitoring’ so that if a rapid heart rhythm does occur this can be transmitted back to your cardiologist through a device like a modem from your home. Generally ICDs should be checked with your cardiologist every 6-12 months to make sure you are well and that no changes to the programming need to be made. A newer ICD called a subcutaneous ICD can also treat patients for dangerously rapid heart beats or a cardiac arrest without having to pass leads through a vein to reach the heart. Instead a lead is passed in front of the sternum (breastbone) to deliver shocks. This device is easier to implant and it may be more suitable for young patients as the ‘lead’ part of the device is more durable over many years. These subcutaneous ICDs don’t have all of the features of a conventional ICD, however, so choosing the right ICD is an important discussion with your cardiologist.